I. Background
Malaria is a common social disease in the world, which greatly affects human health, especially in tropical countries.
In Vietnam, malaria mainly occurs in Central Vietnam and West Highlands. This region is characterized by its difficult natural and socio-economic conditions with the population of over 15 million (making up 17% in comparision with the whole country’s population); the people living in malaria-endemic areas account for 40% of the region’s population and 7.27% of the country’s population. Particularly in 2015, there were 7,644 cases of malaria infection, of which one death from malaria.
The Prime Minister has promulgated the Decision No.1920/QD-TTg dated 27th October 2011 on approving the National Strategy on Malaria Control and Elimination in Viet Nam for the period of 2011-20120 and orientation to 2030 with the general targets including controlling malaria morbidity rate under 0.15 per 1.000 people, malaria mortality rate under 0.02 per 100.000 people; no provinces being in the period of positive malaria control, 40 provinces in the period of preventing malaria from returning, 15 provinces in the period of malaria elimination and 8 provinces in the period of malaria pre-elimination by 2020; striving to eliminate the disease thoughout the country by 2030.
In order to effectively carry out the National Strategy on malaria control and elimination, it is necessary to manage malaria cases right in the first day of detecting them with the application of Remote Sensing (RS) and Geographic Information System (GIS) into the study, control and management of malaria cases in the remote and deep-lying areas; this helps medical staff to forecast and monitor the malaria situation, thereby to take measures to prevent risk of malaria outbreaks, protecting the community’s health. Therefore, the study is conducted by applying geographic information system (GIS) in monitoring malaria patients (MPs) to manage the information of malaria patients and describe some epidemiological characteristics of MPs on the map with the following objectives:
-General objective:
To map and locate malaria cases using geographic information system (GIS) in some districts with high incidence of malaria, Gia Lai province.
-Specific objectives:
1. To position malaria cases based on malaria case reporting forms and geographic information system (GIS) in some districts of Gia Lai province;
2. To promote the link between the determination of malaria case position by GIS and malaria case reporting with the application of some measures in reducing the likelihood of malaria transmission.
II. Study duration and location:
2.1. Study participating units:
-Principal Investigator: Staff of Epidemiology Department of IMPE Quy Nhon;
-Co-Investigators:
1.Provincial Centre of Malariology, Parasitology and Entomology of Gia Lai;
2.District Medical Centers of Krong Pa, Ia Pa, Kong Chro, Äuc Co, K’Bang, Ia Grai, Chu Puh;
3.14 Communal Medical Stations of Krong Pa district.
2.2. Duration:From 31st July 2017 to 7th September 2017
2.3. Location:
Gia Lai province is in the north of West Highlands, which is bounded by Quang Ngai, Binh Dinh and Phu Yen provinces in the east, by Ratanakiri province (Campuchia) in the west, by Dak Lak in the south, by Kon Tum in the north; it is also in artemisin resistance zone (Tier 1).
The study was conducted in 7 district of Gia Lai province, including Krong Pa, Ia Pa, Kong Chro, Äuc Co, K’Bang, Ia Grai, Chu Puh, where malaria-infected cases are always higher in number than other districts of the province and the people have regular forest-related activities such as going into the forest and sleeping in the field-huts.
 |
Figure 1: Administrative map of Gia Lai province |
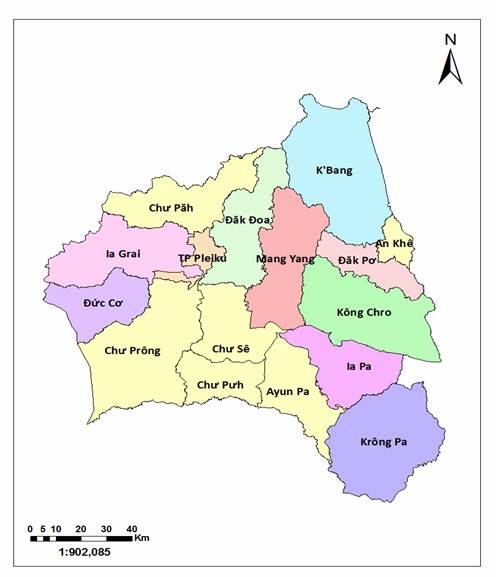 |
Figure 2: Administrative map of the study site |
2.4.Some characteristics of the study site:
2.4.1. Some characteristics of demography and mobility:
-Gia Lai has an area of 15,536.9 km2 and a population of 1,379,730 people (2014) with 34 ethnic groups. As regards natural conditions, Gia Lai has an average elevation of 700-800m above sea level, a cooler climate with two distinct seasons- rainy and dry seasons, of which the rainy season starts in May and ends in October, dry season from November to April the following year. Average temperature is from 22 - 250C.
(Source: http://dulichpleiku.gialai.gov.vn/)
2.4.2. Malaria control network
-The preventive medicine units implementing malaria control include Provincial Centre of Malariology, Parasitology and Entomology, district health centers, communal health stations/ regional polyclinics, village health stations, private health stations, malaria posts (WHO-funded) operating in Krong Pa district, which are not available in the remaining districts.
III. Study objects and methodology:
3.1. Study objects
-GIS map of malaria patient distribution.
-Malaria patients (MPs).
3.1.1. Inclusions:
-Patients diagnosed as malaria sufferers by district medical facilities.
-MPs living or staying in the districts of Krong Pa, Ia Pa, Kong Chro, Duc Co, K’Bang, Ia Grai and Chu Puh.
3.1.2. Exclusions:
-MPs from other places to district medical facilities for diagnosis and treatment.
-Imported MPs.
3.2. Study methodology
The study was designed according to the descriptive research method, using GPS positioning technique combined with the technique of displaying the field measurements into the malaria cases distribution map.
3.3. Sample size
-The retrospective study of all malaria patients (MPs) in the districts of Krong Pa, Ia Pa, Kong Chro, Duc Co, K’Bang, Ia Grai and Chu Puh would be conducted from 2016 to the time of study. The MPs data would be described on the distribution map of malaria cases.
-All MPs would undergo a case investigation and each MP would be determined their living position and suspected location of malaria infection by GIS.
3.4. Steps to proceed:
Krong Pa district was selected by the research team to conduct pre-survey. Three field investigation groups were established. The composition of each survey group included 3 Institute staff members, 1 provincial health worker, 1 district health worker, 1 commune health worker and 1 local pilot.
-Field survey groups would conduct investigation in all 14 communes/towns, in which Group 1 was responsible for 5 communes including Chu Gu, Chu Lao, Ia Rsai, Ia RS, Uar, Team 2 undertook 5 communes/towns of Phu Tuc, Chu Ngoc, Ia Mlah, Dat Bang, Phu Can, and Team 3 was in charge of the remaining 4 communes including Ia Hdreh, Krong Nang, Ia Rmok, Chu Drang.
-From the MPs questionnaire, the research team would develop an electronic MPs questionnaire and upload it to the KLL Collect application. This application runs on Android operating system for mobile devices such as smart phones, tablets, etc. Users interact with the software easily by swiping, sliding, typing text, finger touch, etc.
 |
| Figure 3: The KLL Collect application contains an electronic questionnaire |
-To disseminate the content of data collection forms and the techniques of using the navigation device to each member of each group.
Each field survey group would undertake the following tasks:
-To retrieve data from 2016 to the first 7 months of 2017 at all commune health stations/regional polyclinics, private clinics and district hospitals in Krong Pa district.
-Based on the sampling criteria, the survey groups would classify MPs by group, namely:
+MPs living or working in Krong Pa district.
+MPs from surrounding areas to district medical facilities in Krong Pa district for diagnosis and treatment. These cases would not be included in the study sample because they are in the criteria of exclusion.
-Based on the MPs list, the study team went to each patient's home and conducted face-to-face interviews according to the contents of the MPs questionnaire. This information would be entered into the geographic information system database through the KLL Collect application. The research team would start this application to fully enter the questionnaire information, and activate the GPS positioning function to collect geographic coordinates, altitude of the MPs’ residence places as well as suspected locations of malaria infection (if any). In addition, the KLL Collect application also integrates the imaging function, thereby the team applied this function to snap MPs, MPs’ houses and suspected location of malaria infection.
-After locating the MPs’ residence places, the team would interview the patients to find out the suspected location of malaria infection and move to this location to positioning it and take a photo of the location using mobile device via the KLL Collect application.
-To synchronize collected data (including MPs questionnaire, geographic coordinates of the MPs’ residence places/suspected locations of malaria infection and images) on the geographic information system database (GIS) via Internet connection.
 |
Figure 4: Collected data is synchronized on the malaria case distribution map |
-The position of the MPs identified through investigations of the study groups would be aggregated and displayed on the distribution map of malaria cases.
-After conducting the survey in Krong Pa district, the research team continues to investigate the remaining districts including Ia Pa, Kong Chro, Duc Co, K'Bang, Ia Grai and Chu Pah.
3.5.Data collection techniques:
-Retrospect of MPs data: To use the prepared forms to collect data in medical facilities in Krong Pa district.
-Direct interviews: MPs would be interviewed for relevant epidemiological factors through the prepared questionnaire.
-GPS positioning: To use portable handheld devices with the KLL Collect app installed. KLL Collect is a free application in the CH Play app store. This application has some minimum requirements when installing as follows:
+Running on Android version 4.0.0 or above.
+Minimum memory capacity of the device is 5GB.
+Mobile devices must have built-in GPS.
In order to perform GPS positioning for the MPs’ houses and suspected locations of malaria infection, the research team worked on KLL Collect software in five steps as follows:
Step 1: Go to the CH Play application store (this application store is available in Android smartphones) and download the KLL Collect software, then install it on the device.
Step 2: Create form for electronic data entry, which will be programmed based on the programming language guided by the home page of the KLL Collect software. Then this form will be uploaded to the server created by the research team at https://ona.io
Step 3: Each member of the research team will download the electronic form (questionnaire) from the server of KLL Collect software.
Step 4: The research team will conduct the interview. Upon completion of the interview, investigators will enter data on the electronic data entry form, and turn on the GPS positioning function to record geographic coordinates (latitude, longitude and altitude) and snap 3 photos of the patient's home. Based on the information collected from the patient, the team will determinate the position patients suspected of infecting malaria with the similar procedure performed at the patient's home.
Step 5: After completing the survey, the team will compare the questionnaire and electronic data. If no errors are detected during the investigation, the data will be uploaded to KLL Collect server (created by the research team) via internet connection.
Note: The team leader of the investigation is the only person who manages the account to access the database to ensure the confidentiality of the information collected. The study team members will be provided with additional accounts to collect and send data to the server (sub accounts cannot have access to the database system).
IV. Results of the survey
4.1. MPs’ position on GIS map of malaria patient distribution
4.1.1. GIS map of MPs’ distribution in some districts of Gia Lai province
The survey team has determined the position of malaria cases in seven districts with the highest number of malaria cases in 2017 including Krong Pa, Ia Pa, Kong Chro, Duc Co, Chu Puh, K'Bang and Ia Grai. All malaria cases detected from the beginning of 2017 to the time of study (7 first months of 2017) would be investigated through a case investigation form and be determined their living positions and suspected locations of malaria infection. In the particular case of Krong Pa district, the research team has conducted this activity with a list of malaria patients diagnosed from 2016 to the time of the study.
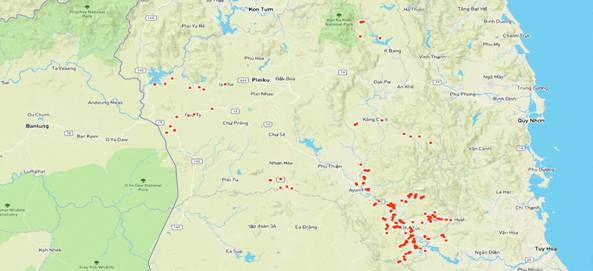 |
Figure 5: Map of 7 districts with the highest number of MPs in Gia Lai province |
Remarks: Figure 5 is a map of malaria cases distribution that utilizes GIS and GPS. This is a basic map of administrative boundaries, rivers, traffic system and altitudes. Each red spot on the map corresponds to one MP into whom the research team has conducted the investigation. The area with many red dots in the south east of the map is Krong Pa district where has a large population of MPs. The reason for higher density of spots in this district than that in the remaining districts is that Kong Pa district has had MPs much more than the other districts, according to the data investigated by the research team from 2016 to the first 7 months of 2017.
 |
Figure 6: Map of 7 districts with the highest number of MPs in Gia Lai province by satellite |
Remarks: Figure 6 is a malaria distribution map with images taken by satellite. In contrast to the basic map shown in Figure 5, the satellite map is the actual image, the vegetation is clearly visible on the map. Therefore, users can see the distribution of MPs located on the map corresponding to the natural habitat such as forests, rivers, streams and lakes.
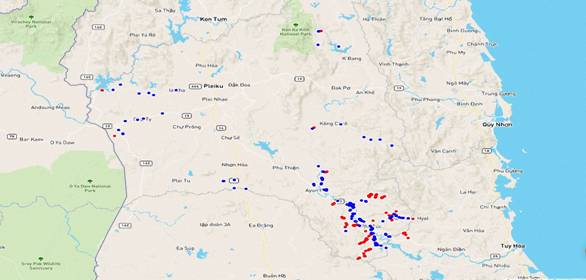 |
| Figure 7: Distribution map of MPs’living locations and malarial sites |
Remarks: The points on the map represent where MPs live and were infected withmalaria in the 7 surveyed districts with the red color corresponding to the suspected locations of malaria infection and blue to the MPs’ habitats.
 |
Figure 8: Distribution map of MPs’living locations and malarial sites by satellite image |
4.1.2. Distribution map of malaria cases in some districts of Gia Lai province
4.1.2.1. Distribution map of malaria cases in Krong Pa district
The research team has conducted the investigation of malaria cases from 2016 to the first 7 months of 2017 throughout Krong Pa district, the cases were described on the distribution map as follows:
 |
Figure 9: Map of MPs’ residence distribution in Krong Pa district |
Remarks: The MPs’ living locations were mainly in two sides of the Ba River valley and one river branch originating from the watershed forest Ia M'Lah. Areas far from river valley are less populated.
 |
Figure 10: Map of MPs’ distribution by living places in Krong Pa district via satellite |
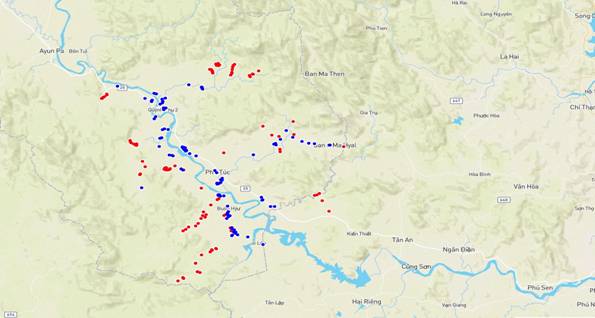 |
Figure 11: Distribution map of MPs’ living locations and malarial sites in Krong Pa district |
 |
Figure 12: Distribution map of MPs’ living locations and malarial sites in Krong Pa district |
Remarks: The points on the map indicate the MPs’ residence and malaria-infected places in the communes of Krong Pa district with the red color corresponding to suspected places of malaria infection and blue to the living places of patients. Suspected locations of malaria infection are mainly concentrated in three clusters that are circled yellow on the map. Cluster 1 is of the forestal area Ia RSai - Churam, cluster 2 is of the watershed area Ia M'Lah, cluster 3 is of the conservation forest Ea So.
4.1.2.2. Distribution map of malaria cases in Duc Co district
 |
Figure 13: Distribution map of MPs’ living locations and malarial sites in Duc Co district |
Remarks: The distribution of MPs’ residence were mainly found in Ia Dom and Ia Nam communes, this population group has forest-involved activities in the border area with Rattanakiri province (Cambodia). on the map, the red dots represent the locations where MPs went to for forestal work following the yellow arrow, and the MPs’ locations near the border between Vietnam - Cambodia are black.
4.1.2.3. Distribution map of malaria cases in Chu Puh district
 |
Figure 14: Distributionmap of MPs’ living locations and malarial sites in Chu Puh district |
Remarks: The MPs were mainly found in Ia Le and Ia B'Lu communes. This group has forest-involved activities in Duc Co district, where has the border with Cambodia.
4.1.2.4. Distribution map of malaria cases in Ia Grai district
 |
Figure 15: Distribution map of MPs’ living locations and malarial sites in Ia Grai district |
Remarks: The MPs were found in many communes of the district. This group has forest-involved activities near the watershed area where the Se San 4 hydropower plant is located. on the map, the red dots represent the locations where MPs went to for forestal work following the yellow arrow.
4.1.2.5. Distribution map of malaria cases in Ia Pa district
 |
Figure 16: Distribution map of MPs’ living locations and malarial sites in Ia Pa district |
Remarks: The MPs were mainly found in Ia K’Dam commune. This group has forest-involved activities in the forestal area of Ia K’Dam. on the map, the red dots represent the locations where MPs went to for forestal work following the yellow arrow.
4.1.2.6. Distribution map of malaria cases in K’Bang district
Figure 17: Distribution map of MPs’ living locations and malarial sites in K’Bang district
Remarks: The MPs were mainly found in Kroong commune. This group has cultivation activities in their residence places. on the map, the red dots represent the locations where MPs went to for cultivation following the yellow arrow.
4.1.2.7. Distribution map of malaria cases in Kong Chro district
 |
Figure 18: Distribution map of MPs’ living locations and malarial sites in Kong Chro district |
Remarks: The MPs were found in many communes of the district, mainly in Dak Pling commune. This group has forest-involved activities in the forestal area of Meo village, Dak Pling commune. on the map, the red dots represent the locations where MPs went to for forestal work following the yellow arrow.
4.2. Analysis of some MPs’ epidemiological characteristics
4.2.1. Some demographic characteristics of the investigated patient group
The research team has carried out the investigation of 171 malaria cases in 7 districts of Krong Pa, Ia Pa, Kong Chro, Duc Co, Chu Puh, K'Bang, Ia Grai from 2016 to the first 7 months of 2017. Several reasons for incomplete investigation of the MPs are that MPs from other districts in the province or districts outside the province go to district medical facilities for treatment, patients move to other places for settlement (getting married, going to the south for work, etc.), some patients’ names in the medical records of district hospital cannot be found at the locality, some cases are duplicated, etc.
Table 4: Demographic characteristics of the investigated patient group
No. | Variable | Value | Quantity | % |
1 | Age | < !important;5 | 3 | 1,75 |
5-15 | 22 | 12,87 |
> !important;15 | 146 | 85,38 |
2 | Gender | Male | 149 | 87,13 |
Female | 22 | 12,87 |
3 | Ethnic group | Jrai | 127 | 74,27 |
Kinh | 29 | 16,96 |
Bana | 13 | 7,60 |
Muong | 1 | 0,58 |
Tay | 1 | 0,58 |
4 | Career | Farmer | 142 | 83,04 |
Others | 29 | 16,96 |
Remarks: The demographic characteristics of the study subjects are as follows: Among 171 surveyed MPs, people over 15 years old dominate with 85.38%, most of them are male and farming is the main occupation. The Jrai ethnic group accounted for 74.27% of the total surveyed malaria cases.
Table 5: Places of detecting MPs
No. | Place | Quantity | % |
1 | District hospital | 56 | 32,75 |
2 | Commune health station | 112 | 65,50 |
3 | Epidemiological Survey | 2 | 1,17 |
4 | Private healthcare | 1 | 0,58 |
Remarks: MPs were mainly detected at commune health station with 65.50%. However, the district hospital also detected and treated about 32.75% of the patients who went directly to this place for medical examination. Private healthcare services also found MPs with very low rate of 0.58%.